Why Precocious Puberty Is an Enemy of Height
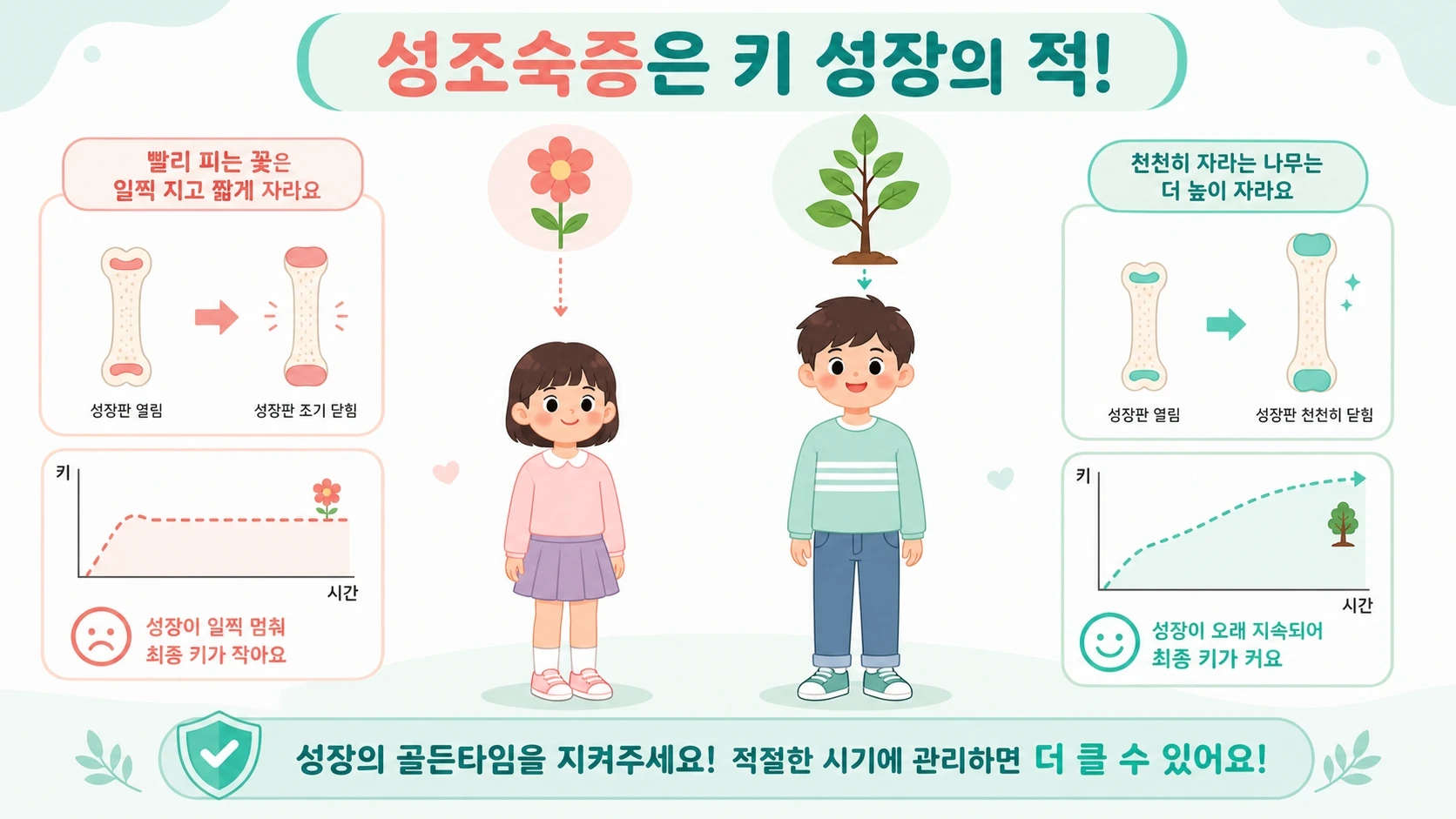
Precocious puberty stunted growth is one of the most concerning — yet frequently misunderstood — outcomes parents face when their child enters puberty too early. Under normal circumstances, children grow at a steady, predictable pace from birth until the pubertal growth spurt kicks in, when sex hormones can drive gains of 7–12 cm per year. At the end of puberty those same hormones signal the growth plates to fuse, ending height gains for good.
Precocious puberty is defined as puberty onset before age 8 in girls and before age 9 in boys. When sex hormones surge years ahead of schedule, the body receives the "close the factory" signal far too soon — before the child has had enough time to build toward their full genetic potential. That premature hormonal exposure is the central mechanism behind precocious puberty and short stature, and it explains why catching it early matters so much.
Growth Plates 101: The Biological Clock Behind Height
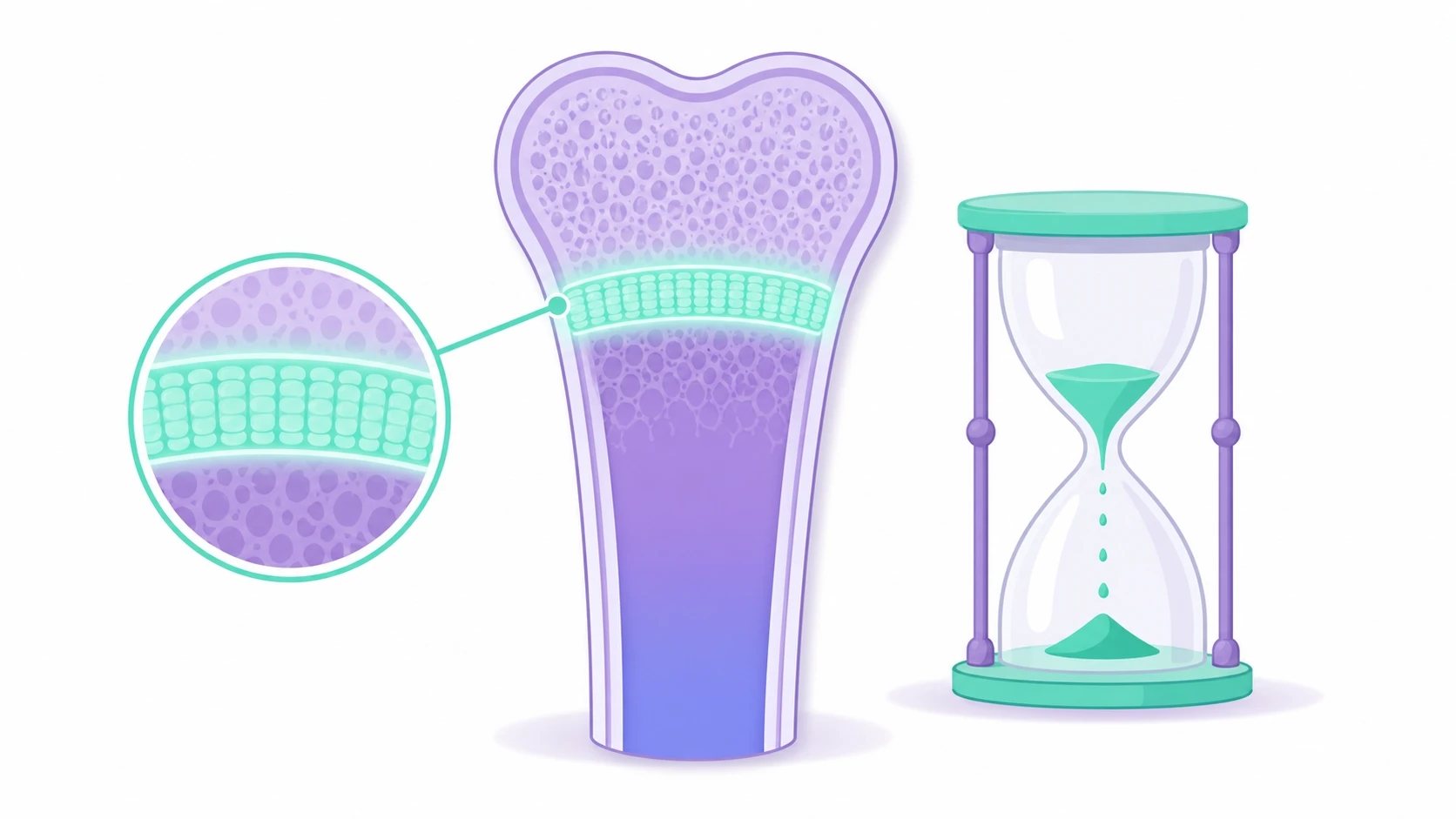
At the end of every long bone in the body sits a thin layer of cartilage called the growth plate (epiphyseal plate). New bone cells are constantly produced here, pushing the bone longer and the child taller — think of it as a silent construction site running around the clock. As long as growth plates stay open and active, height gains are possible.
When puberty begins, the initial surge of estrogen and testosterone actually accelerates plate activity, producing the dramatic growth spurt. But those same hormones also trigger a second, slower process: converting the flexible cartilage into rigid bone. In a normal pubertal timeline, this ossification happens gradually after the child has already captured years of growth. Early puberty growth plate closure cuts that runway short. The construction site shuts down before the building is finished, and once the plates are fully fused, no treatment can reopen them.
The Misleading Growth Spurt: Tall Now, Short Later
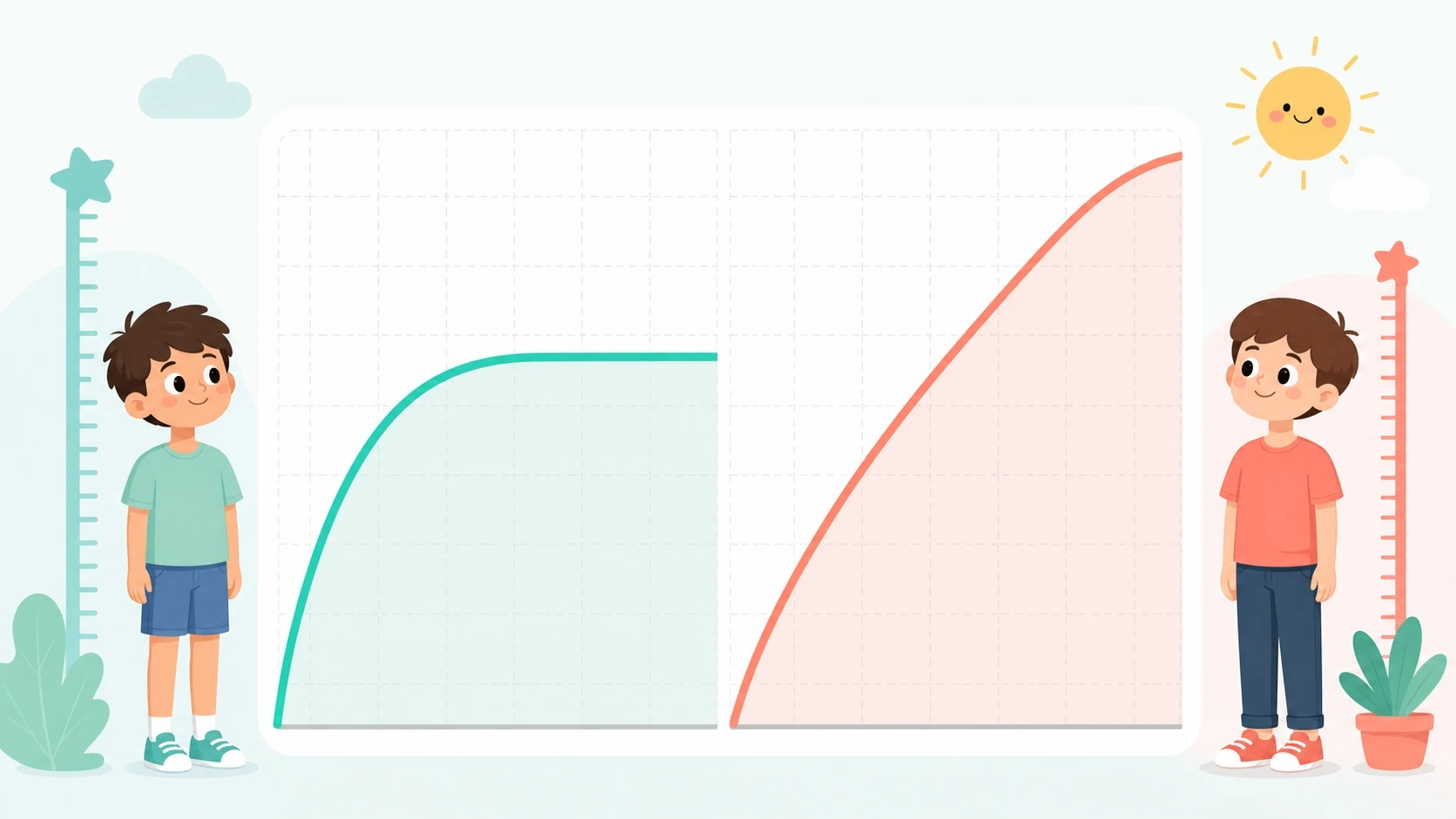
One of the trickiest aspects of precocious puberty and short stature is that the problem disguises itself as a benefit at first. Children with early puberty frequently shoot up faster than their classmates in early elementary school, appearing tall for their age. Parents sometimes take this as reassurance that nothing is wrong — but the growth chart tells a more complicated story.
Because early puberty stops growth far sooner than normal, those children plateau while their peers are still in the middle of their own growth spurts. A child who looked above average at age 8 may be overtaken by every classmate by age 12, when their growth plates have already fused and further gains are no longer possible. Studies consistently show that untreated precocious puberty can reduce final adult height by several centimeters compared to the child's genetic target height — a gap that cannot be recovered once the window closes.
Recognizing the Warning Signs Early
Knowing what to watch for is the first practical step in preventing precocious puberty stunted growth from affecting your child's final height. In girls, the most common early sign is breast budding — a small, sometimes tender disc of tissue beneath the nipple — appearing before age 8. Pubic or underarm hair, accelerated bone growth, and body odor can accompany it. In boys, testicular enlargement before age 9, followed by pubic hair and a deepening voice, are the hallmark signals.
Parents often assume that a child who "looks older" is simply developing normally. However, if any of these signs appear significantly ahead of the typical age range, a bone age X-ray is the fastest way to gauge how much growing time remains. A bone age that runs 1–2 years ahead of chronological age is a red flag that early puberty growth plate closure may already be underway and that specialist evaluation is warranted without delay.
What a Growth Specialist Can Do

If early puberty is confirmed, a pediatric growth specialist will typically start with a bone age assessment — an X-ray of the left hand and wrist compared against standardized reference charts — to estimate how many centimeters of growth potential remain. Blood tests for LH, FSH, and sex hormone levels help confirm whether the process is truly central (driven by the brain's GnRH axis) or peripheral (caused by an external hormone source such as a tumor or exogenous exposure).
For central precocious puberty, GnRH analog therapy is the established medical approach to pause the hormonal cascade and allow growth plates to remain open longer, effectively buying the child more time on the height timeline. Integrated clinics experienced in treating precocious puberty and short stature combine this with bone age monitoring, nutritional guidance, and sleep and lifestyle coaching — because no single intervention works in isolation. Parents who notice early signs and seek evaluation promptly consistently achieve better outcomes than those who wait and watch.
Lifestyle Factors That Can Make Early Puberty Worse
Medical treatment addresses the hormonal mechanism, but several everyday lifestyle factors are known to either accelerate or moderate the onset of puberty. Excess body fat is one of the most researched contributors: adipose tissue converts androgens into estrogen, raising circulating hormone levels and nudging the puberty clock earlier — a key reason why childhood obesity is independently linked to early puberty stops growth concerns in girls especially.
Environmental hormone disruptors — found in certain plastics (BPA), pesticides, and personal care products — are another documented risk factor. Limiting exposure by choosing BPA-free containers, washing produce thoroughly, and reviewing ingredient lists on children's shampoos and lotions is a practical preventive step any family can take. A diet low in processed foods and high in fiber, combined with regular moderate exercise and consistent sleep schedules, supports healthy hormone balance and helps protect the growth window even in children who are genetically predisposed to earlier development.
FAQ
Does precocious puberty always lead to stunted growth?
Not inevitably, but it significantly raises the risk. Without any intervention, children with central precocious puberty often end up shorter than their predicted genetic height because early puberty stops growth by closing the growth plates ahead of schedule. How much height is lost depends on how early puberty starts, how advanced bone age is at diagnosis, and whether treatment is started promptly. Early evaluation is the best way to assess individual risk.
My daughter is 7 and developing breast buds — should I be worried?
Breast development before age 8 in girls is one of the defining criteria for precocious puberty and warrants a medical evaluation rather than a wait-and-see approach. A bone age X-ray and hormone blood panel can quickly determine whether the development is truly early puberty or a benign variation called premature thelarche. Getting clarity early preserves the most treatment options if early puberty growth plate closure is confirmed.
Can GnRH analog treatment fully restore a child's lost height potential?
GnRH analogs work best as a preventive tool — they pause the hormonal cascade to protect growth time that has not yet been lost. If treatment starts before significant bone age advancement, outcomes are generally good and final height can be close to the genetic target. However, GnRH analogs cannot reopen growth plates that have already fused. This is why early diagnosis and timely specialist referral are the most important factors in managing precocious puberty and short stature effectively.
References
- Precocious puberty and statural growth. Human reproduction update. 2004. PubMed · DOI
- Central precocious puberty: current treatment options. Paediatric drugs. 2005. PubMed · DOI
- Predictors of bone maturation, growth rate and adult height in children with central precocious puberty treated with depot leuprolide acetate. Journal of pediatric endocrinology & metabolism : JPEM. 2018. PubMed · DOI
- Using change in predicted adult height during GnRH agonist treatment for individualized treatment decisions in girls with central precocious puberty. Journal of pediatric endocrinology & metabolism : JPEM. 2023. PubMed · DOI
- Final height after gonadotrophin releasing hormone agonist treatment for central precocious puberty: the Dutch experience. Journal of pediatric endocrinology & metabolism : JPEM. 2000. PubMed · DOI