What Are Growth Plates and Why Do They Matter?
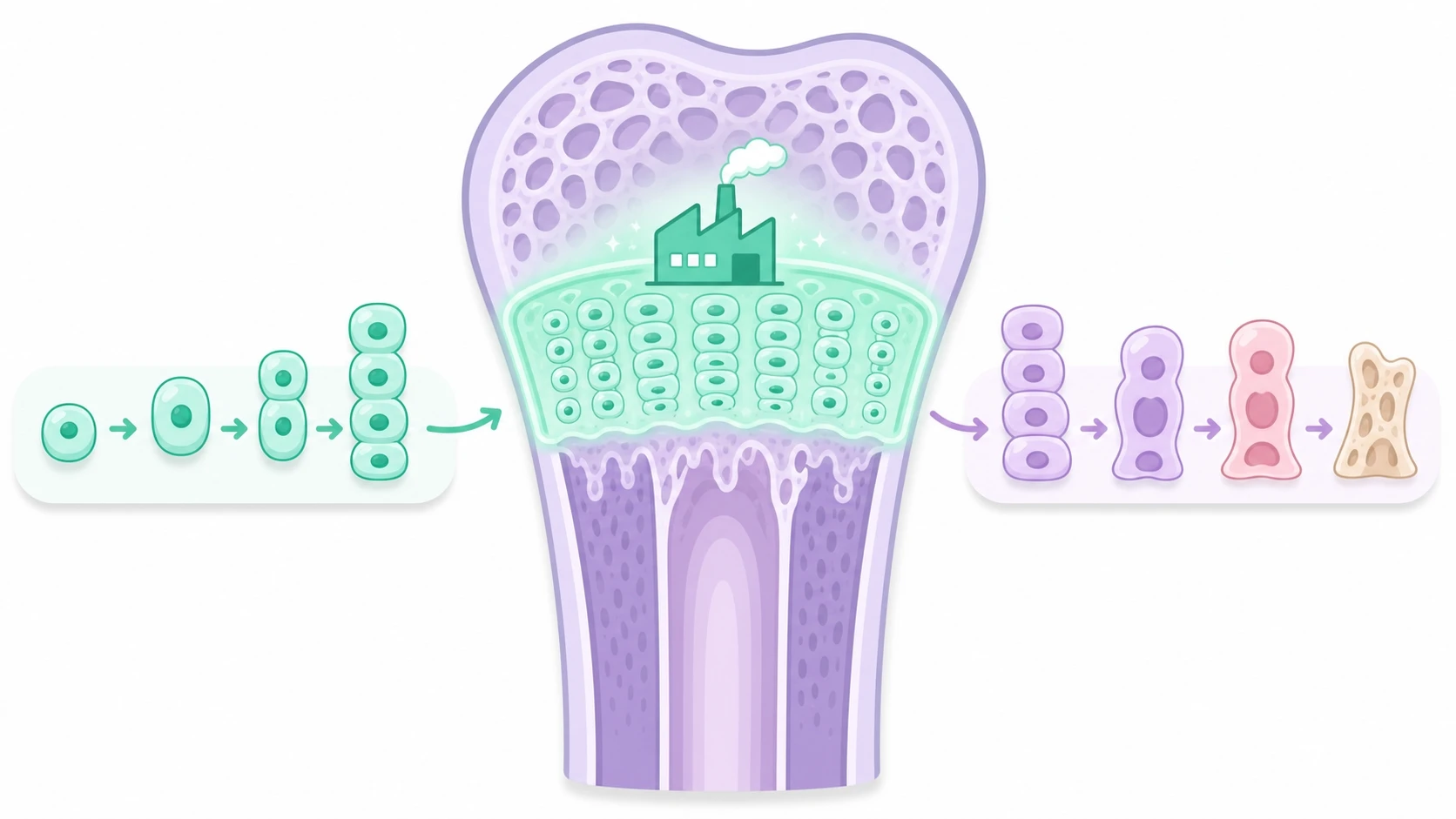
Growth plate closure age is one of the most important concepts parents should understand when thinking about their child's height potential. Growth plates — also called epiphyseal cartilage — are thin layers of developing cartilage tissue located near the ends of long bones. These zones contain rapidly dividing cells that continuously produce new bone, allowing a child's skeleton to lengthen and their body to grow taller over time.
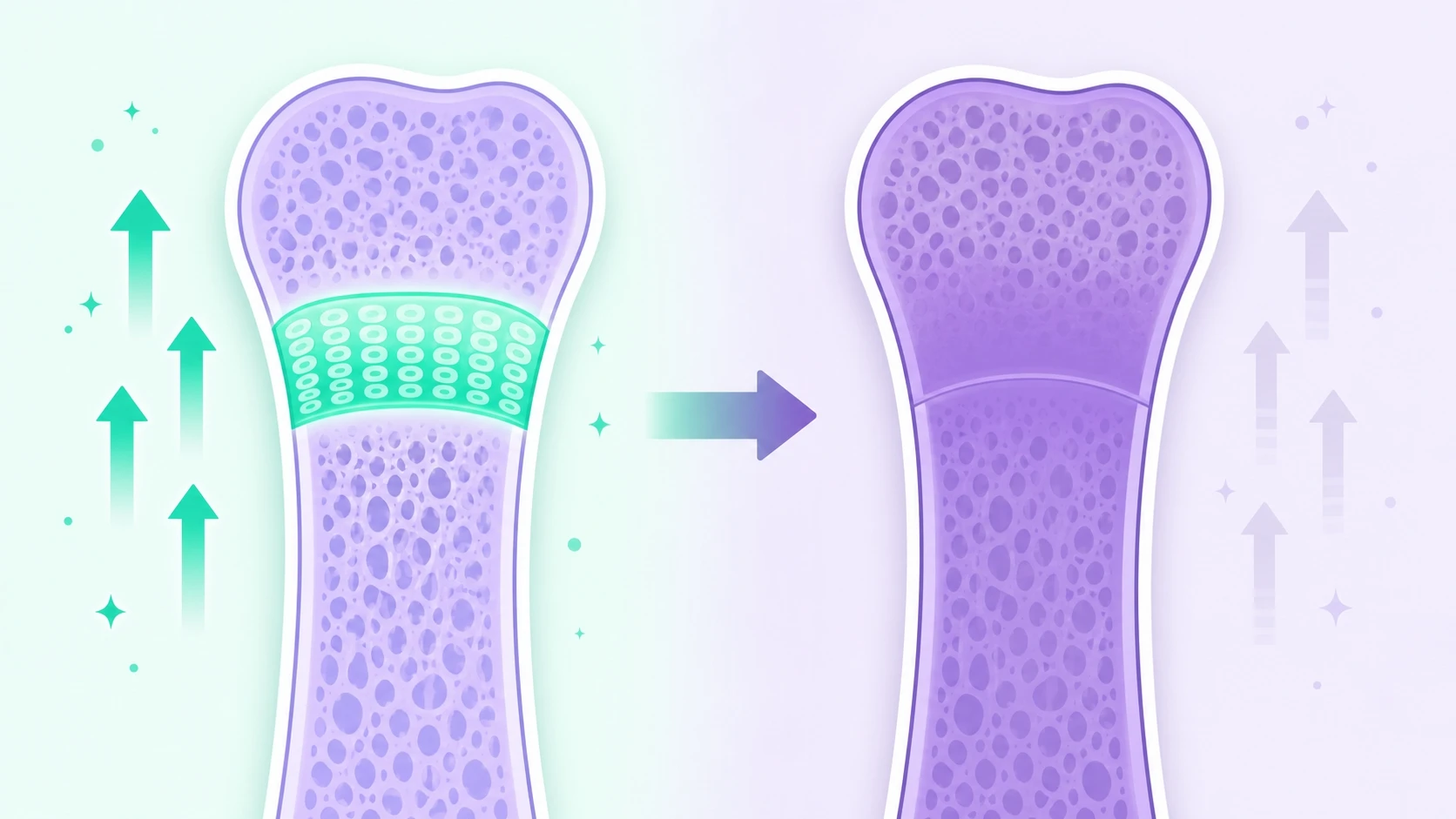
Think of each growth plate as a small manufacturing facility dedicated to building bone. As long as the facility stays open, bone production continues. During puberty, however, rising sex hormone levels gradually cause this cartilage tissue to ossify — to harden into solid bone — a process known as growth plate fusion or closure. Once a growth plate has fully closed, no further lengthening of that bone can occur, which means height growth in that segment of the body is permanently complete.
Understanding when this process happens — and what influences its timing — gives parents and clinicians a meaningful opportunity to support a child's growth while the window is still open.
Growth Plate Closure Age in Girls: What to Expect
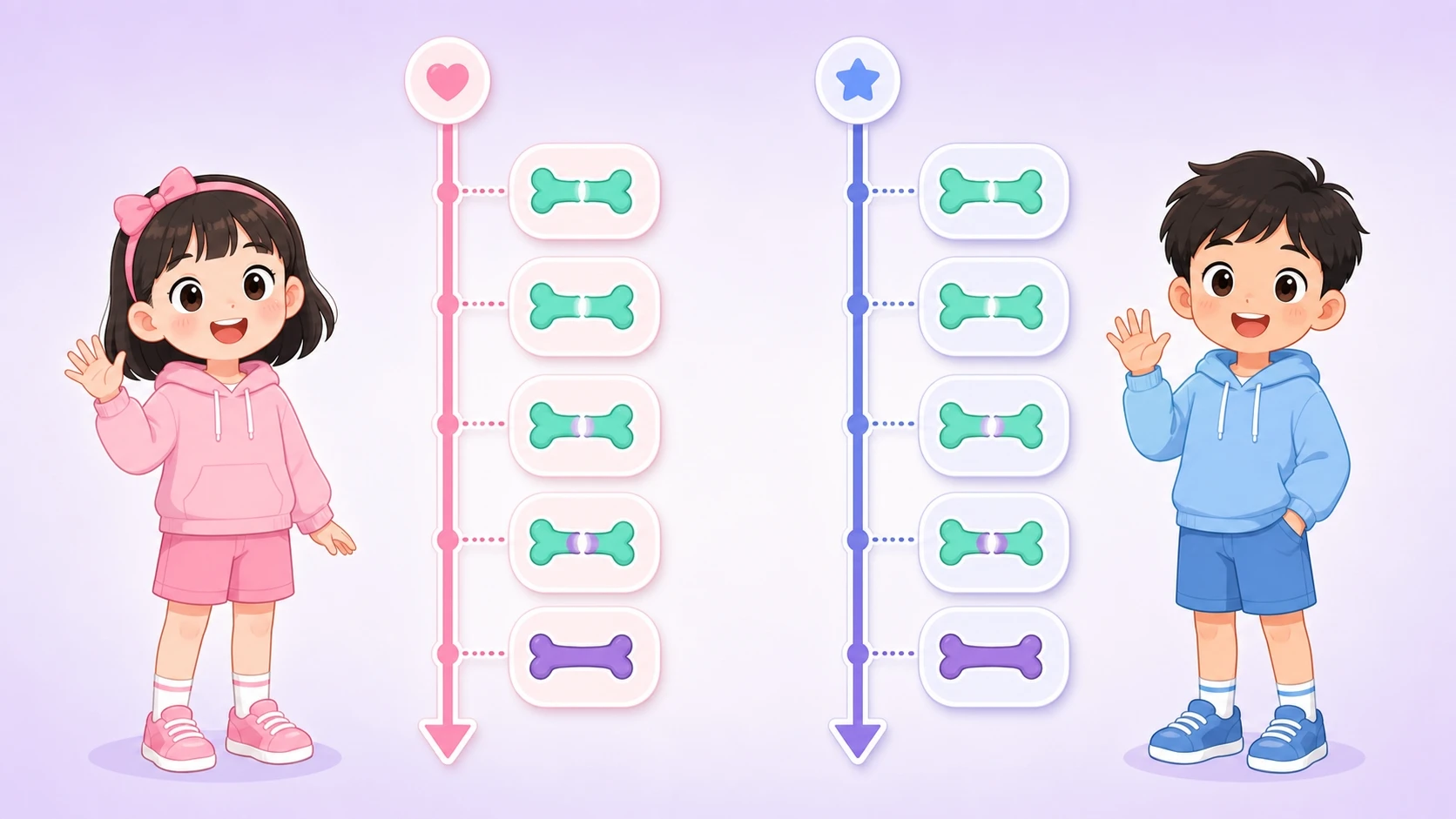
Understanding when do growth plates close in girls requires looking at the puberty timeline. Girls typically enter puberty about one to two years earlier than boys, with the first signs — such as breast development — appearing around age 10 on average. This earlier hormonal shift means the closure process also begins sooner.
Estrogen plays a dual role in female growth: at moderate concentrations it stimulates the growth plates, but as levels rise higher during mid-to-late puberty, estrogen accelerates closure. As a result, the growth rate slows sharply after the first menstrual period. Most girls continue to gain height for about two to three years after menarche, but in noticeably smaller increments each year.
By around ages 14 to 16, the majority of a girl's growth plates have fused. Individual variation exists — girls who enter puberty earlier tend to close their growth plates earlier, while late developers may retain open plates into their mid-teens. Monitoring bone maturity alongside chronological age is the most reliable way to assess how much growing time remains.
Growth Plate Closure Age in Boys: A Later Timeline
When do growth plates close in boys? Because male puberty typically begins one to two years later than in girls — with the first signs such as testicular enlargement appearing around ages 11 to 12 — the entire growth trajectory shifts later. Boys also experience a longer and more intense growth spurt, often gaining height more rapidly at peak velocity than girls do.
Testosterone, like estrogen, initially promotes bone lengthening by stimulating the growth plates, then at higher concentrations triggers their gradual fusion. Because testosterone levels rise on a later schedule, boys generally retain open growth plates longer, allowing more cumulative time for height gain.
Most boys reach full growth plate closure between ages 16 and 18, with some late developers extending slightly beyond that range. This two-year difference compared to girls is why the average adult male is taller than the average adult female, even when parental heights are similar. If parents notice their son seems shorter than peers at age 14 or 15 but puberty has not yet fully progressed, remaining growth potential may still be substantial.
Growth Plates Close at Different Times in Different Parts of the Body
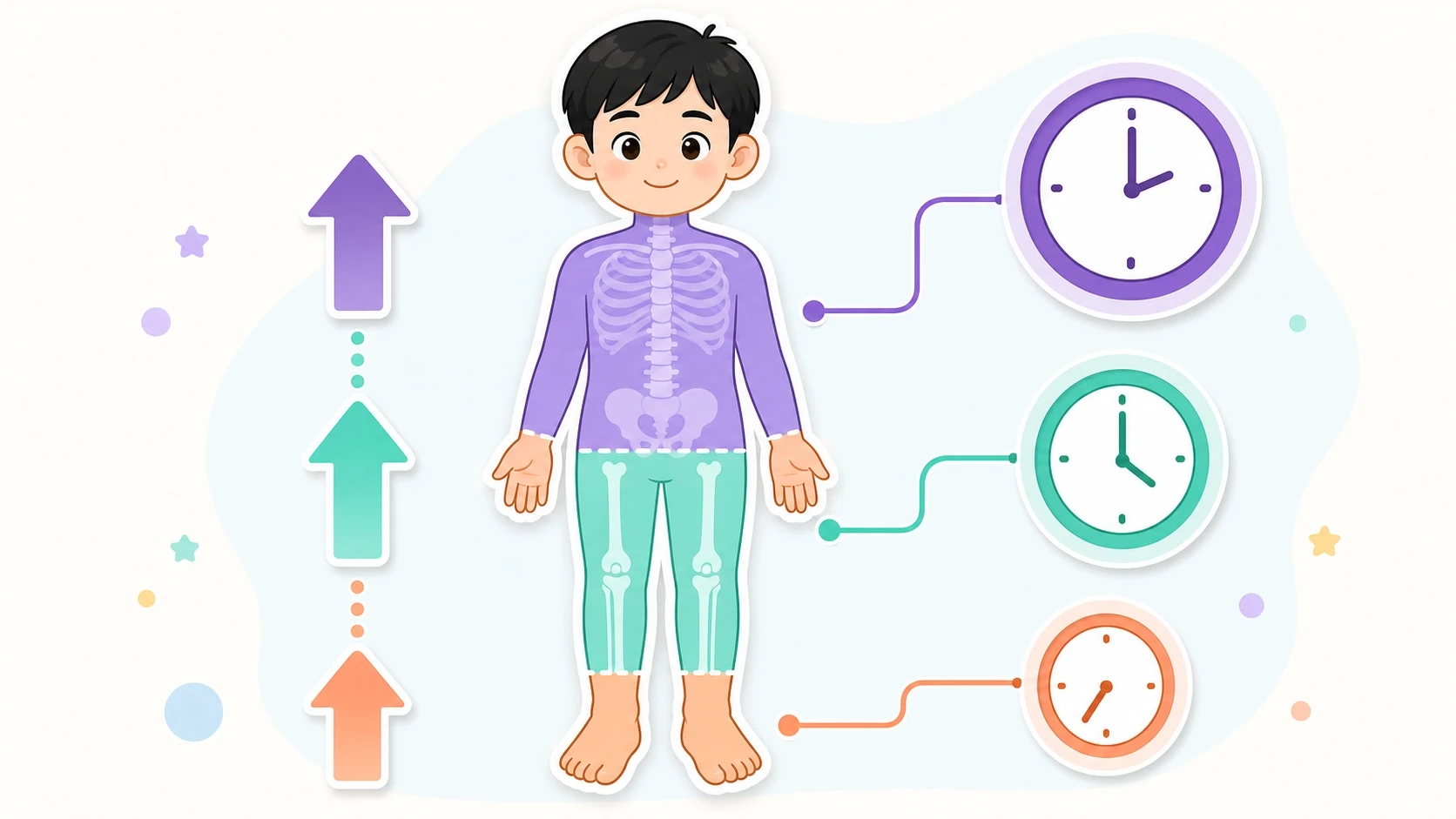
Growth plates do not close all at once across the skeleton. The process follows a predictable anatomical sequence, moving generally from the extremities inward and from the lower body upward.
Hands and feet. The small bones in the fingers and toes contain some of the first growth plates to fuse. Because these sites close relatively early, their bone maturity level is a useful early signal of overall skeletal status.
Knee growth plates. The growth plates at the lower end of the femur (thigh bone) and the upper end of the tibia (shin bone) are among the most important for overall height, as the legs contribute a large proportion of stature. These plates typically fuse slightly later than those in the hands and feet. When the knee growth plates are confirmed closed on imaging, most of a child's height gain is complete.
Spinal growth plates. The vertebral end plates are among the last to fully fuse in the entire skeleton. Even after the knee growth plates have closed, a small additional increment — typically one to two centimeters — may still occur through continued spinal maturation. This is why posture and spinal health remain relevant even in later adolescence.
How a Growth Plate X-Ray Helps Assess Remaining Growth

A growth plate x-ray — most commonly taken of the left hand and wrist — is the standard clinical tool for determining a child's bone age, which measures skeletal maturity rather than calendar age. Radiologists compare the size, shape, and fusion status of the small wrist and hand bones to established reference charts to assign a bone age in years and months.
Bone age is valuable because it often differs meaningfully from chronological age. A child who is 10 years old by birthday but has a bone age of 12 has a skeleton that is maturing faster than average, suggesting growth plate closure may arrive earlier than expected. Conversely, a bone age of 8 in that same 10-year-old indicates the skeleton is developing more slowly, which generally means more growing time remains.
Combining bone age with current height and parental heights allows a pediatric growth specialist to estimate predicted adult height with reasonable accuracy and to assess whether a child is on track, ahead, or behind their expected trajectory. A growth plate x-ray is non-invasive, takes only a few minutes, and provides information that no questionnaire or physical observation alone can supply.
Making the Most of the Window Before Growth Plates Close

The most important takeaway for parents is that growth plate closure age is not a fixed destiny — it is a window, and what happens inside that window matters enormously. Several evidence-supported lifestyle factors influence how well a child grows during the open-plate years.
Sleep. The majority of daily growth hormone secretion occurs during deep sleep, making consistent, high-quality rest one of the highest-leverage habits for any growing child. School-age children generally need nine to eleven hours per night.
Physical activity. Load-bearing and rhythmic exercises such as jumping, swimming, and running stimulate growth plate activity and improve overall bone density. Sedentary habits, by contrast, reduce the mechanical signals that encourage bone growth.
Nutrition. Protein, calcium, and vitamin D are the primary nutritional pillars of bone development. Diets high in processed foods and added sugar can interfere with growth hormone metabolism and, in some research contexts, accelerate early puberty onset — effectively shortening the available growth window.
If a child's bone age is advancing faster than expected, or if height velocity has slowed significantly, consulting a pediatric growth specialist allows for a structured assessment and, where appropriate, a personalized plan to support remaining growth potential before the plates close.
FAQ
Can you tell if growth plates are closed without an x-ray?
Not reliably. While certain physical signs — such as the completion of puberty milestones or a height that has not changed in over a year — suggest plates may be closing, the only accurate way to assess growth plate fusion status is through a bone age x-ray of the hand and wrist, interpreted by a trained clinician.
Does early puberty mean growth plates close earlier and final height is shorter?
In general, yes. Earlier puberty triggers an earlier rise in sex hormones, which accelerates growth plate maturation and fusion. Children who enter puberty significantly ahead of their peers often experience a shorter total growth window, which can result in a lower final adult height than their genetic potential would otherwise suggest. Early assessment by a growth specialist can help determine whether intervention is appropriate.
Is there anything that can be done once growth plates are partially closed?
Once a growth plate has fully fused, that bone cannot lengthen further. However, partial closure does not mean all growth has ended — other growth plates across the skeleton, including spinal end plates, may still be open. The key is accurate assessment: a bone age x-ray identifies which plates remain active, and a specialist can advise on whether lifestyle optimization or medical evaluation is warranted given the remaining time.
References
- Validation of bone age methods by their ability to predict adult height. Hormone research in paediatrics. 2010. PubMed · DOI
- Prediction of adult height based on automated determination of bone age. The Journal of clinical endocrinology and metabolism. 2010. PubMed · DOI
- Prediction of adult height using maturity-based cumulative height velocity curves. The Journal of pediatrics. 2005. PubMed · DOI
- Aromatase Inhibitors Treatment Alone or With GH Increases Final Height in Short-statured Pubertal Boys-Real-world Data. The Journal of clinical endocrinology and metabolism. 2025. PubMed · DOI
- Inhibition of estrogen biosynthesis with a potent aromatase inhibitor increases predicted adult height in boys with idiopathic short stature: a randomized controlled trial. The Journal of clinical endocrinology and metabolism. 2006. PubMed · DOI