The Growth Paradox Every Parent Should Know
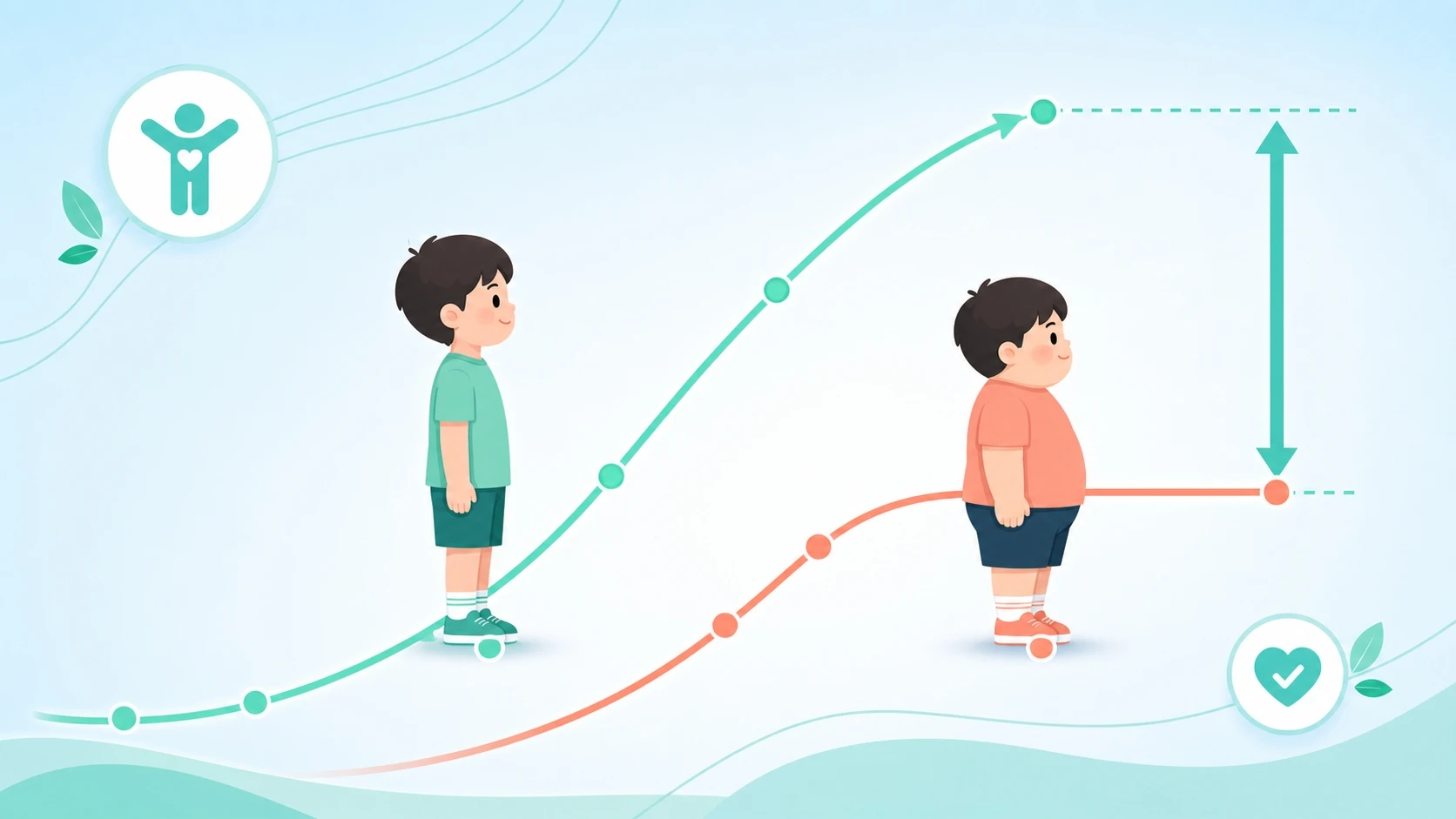
The link between childhood obesity and early puberty catches many parents off guard. When a heavier child appears taller than classmates, the natural reaction is reassurance — surely the extra size means everything is fine. In reality, pediatric growth specialists observe the opposite pattern every day: overweight children often grow faster in the short term, yet finish shorter as adults than their leaner peers. This is not a contradiction; it is a predictable outcome of how excess body fat disrupts the hormonal signals that govern the growth plates. Understanding this paradox early gives parents a genuine window to act before growth potential is lost.
How Insulin and IGF-1 Drive Temporary Growth in Overweight Children
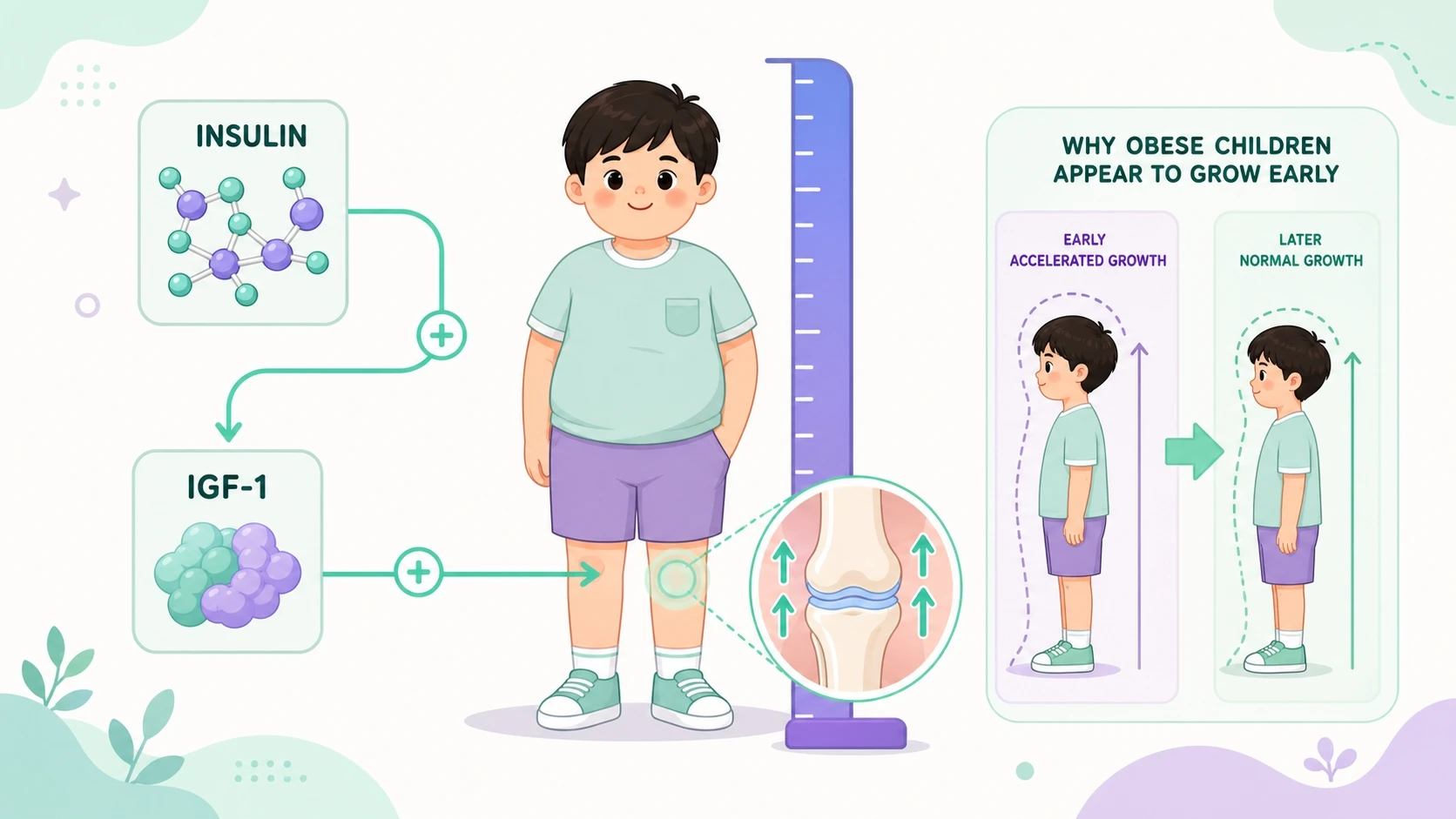
Excess body fat is not simply stored energy — it actively reshapes the body's metabolic environment. In overweight children, puberty-related hormone disruptions can begin well before any visible puberty signs appear. The mechanism starts with insulin resistance: as fat accumulates, cells respond less effectively to insulin, so the pancreas compensates by producing more. This state of elevated insulin (hyperinsulinemia) directly stimulates growth plate cells, producing a noticeable but deceptive surge in height.
Alongside insulin, the liver produces higher levels of IGF-1 (insulin-like growth factor-1) in children carrying excess weight. IGF-1 accelerates the proliferation and differentiation of growth plate cartilage cells, adding to bone length. Leptin, another hormone secreted in larger quantities by fat tissue, can also influence growth plate activity. The combined effect of these hormones makes heavier children appear to be growing well ahead of schedule — a reassuring sight that can mask a brewing problem.
Fat Cells, Estrogen, and the Premature Closing of Growth Plates
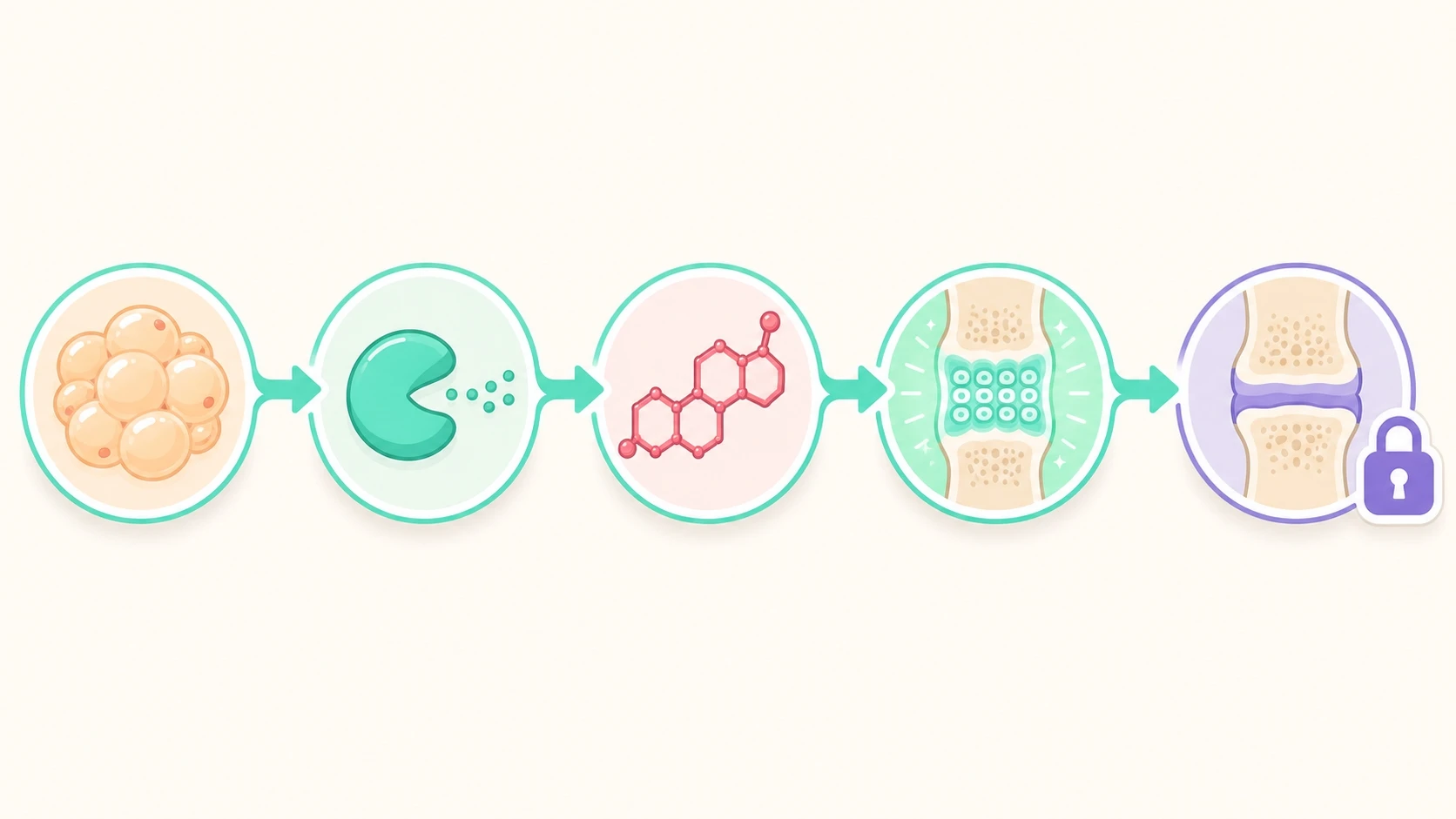
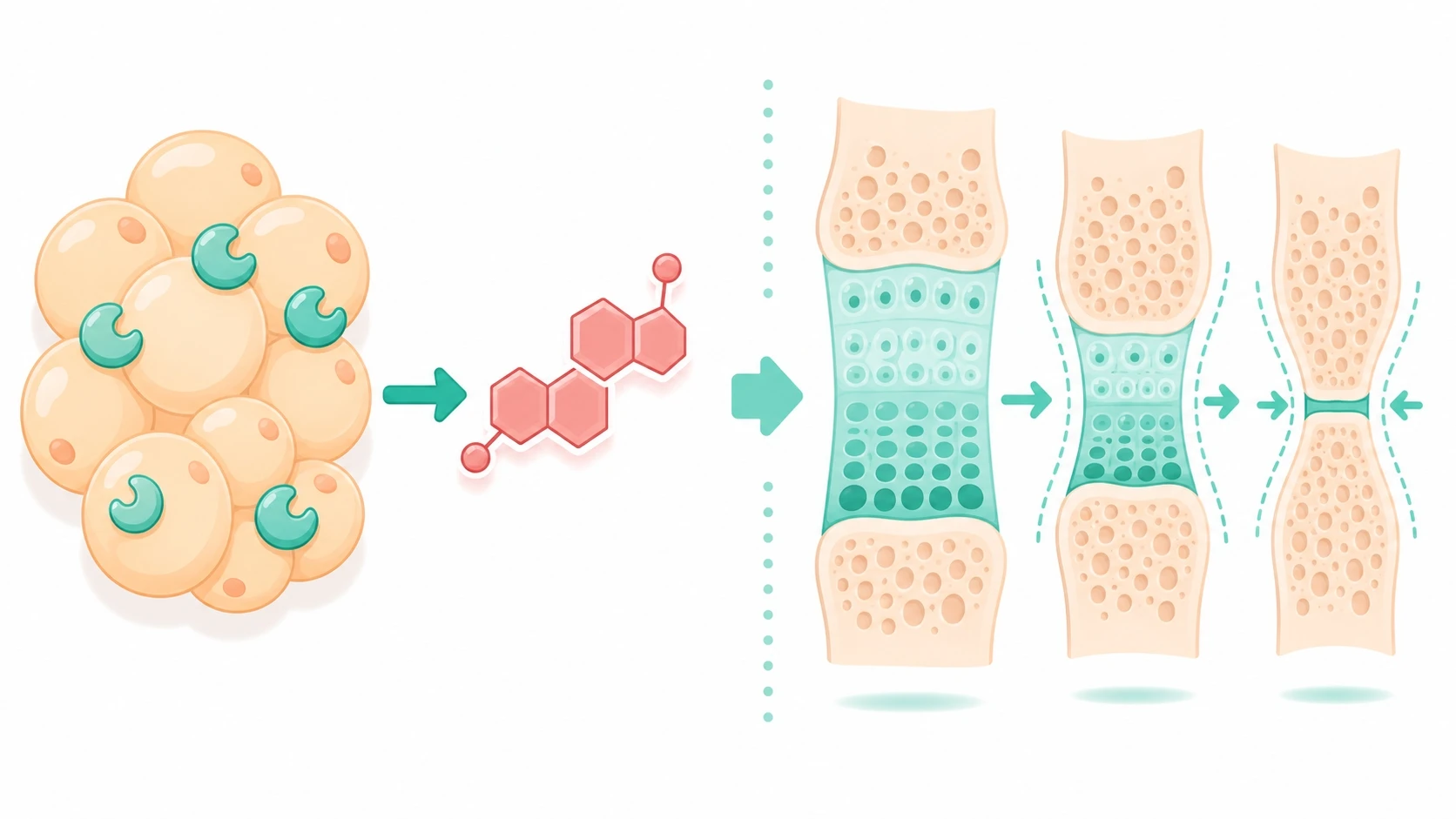
The mechanism that transforms early tallness into a shorter adult height centers on fat cells and estrogen production. Adipose (fat) tissue contains an enzyme called aromatase, which converts androgens (male-type hormones present in both sexes) into estrogen. The more fat tissue a child carries, the more aromatase activity occurs, and the higher the circulating estrogen level — regardless of the child's sex.
Estrogen has two opposing effects on the skeleton. In moderate amounts it supports normal bone growth; in excess it sends a premature signal to the growth plates to close. When bone age races ahead of chronological age, the window for height gain narrows rapidly. This accelerated bone maturation is the biological engine behind obesity precocious puberty in girls (and, less commonly, in boys): secondary sexual characteristics appear earlier than expected, growth plates seal ahead of schedule, and the child's final adult stature ends up lower than genetic potential would predict. Put simply, the body borrows against future height and spends it all at once.
Beyond Height: Metabolic and Psychological Consequences
The consequences of childhood obesity and early puberty extend well beyond a centimeter shortfall in adult height. Children who enter puberty prematurely face elevated long-term risks for insulin resistance, type 2 diabetes, hypertension, and cardiovascular disease — conditions that can compound the metabolic disruption that triggered early puberty in the first place. The cycle is self-reinforcing.
There is also a meaningful psychological dimension. A child who visibly develops earlier than classmates — particularly girls showing breast development at age 7 or 8 — may face confusion, social comparison, and emotional distress at an age when they lack the maturity to process those experiences. Awareness and timely support from parents can soften this impact, but it underscores why early identification matters beyond the clinical picture of bone age and growth curves.
What Parents Can Do Starting Today

Preventing or reversing the effects of overweight on a child's growth requires more than a focus on the scale. Four evidence-supported habits address the underlying hormonal environment:
- Reduce ultra-processed foods and added sugars. High-sugar diets spike insulin repeatedly and can accelerate the hormonal cascade described above. Prioritize vegetables, lean protein, and whole-food carbohydrates at every meal.
- Encourage at least 60 minutes of outdoor physical activity daily. Weight-bearing movement supports healthy bone development and helps regulate insulin sensitivity. Activities such as jumping rope, swimming, and team sports are particularly well-suited to this age group.
- Protect sleep. Growth hormone is secreted most abundantly during deep sleep. Children aged 6–12 need 9–11 hours; teenagers need 8–10. Consistent bedtimes and a screen-free wind-down routine are practical starting points.
- Track growth trends, not just single measurements. A child growing more than expected for their age — especially if early puberty signs appear — warrants a conversation with a healthcare professional who can assess bone age and evaluate growth plate status.
When to Seek a Professional Growth Evaluation
Some warning signs suggest the hormonal disruption has already progressed and warrant professional assessment sooner rather than later. Consider consulting a pediatric growth specialist if your child is noticeably taller than classmates of the same age and sex but seems to be slowing down compared to the previous year, if breast development or pubic hair appears before age 8 in girls or before age 9 in boys, or if a recent bone age X-ray showed skeletal maturation significantly ahead of the child's actual age.
A specialist can measure bone age accurately, evaluate whether growth plates remain open, and assess circulating hormone levels. With that information, a personalized approach — which may include lifestyle coaching on nutrition, activity, and sleep, or where clinically appropriate, medical evaluation for precocious puberty — can be mapped out. The earlier the assessment, the more options remain available.
FAQ
Why do overweight children often appear taller than their peers at first?
Excess fat tissue raises insulin, IGF-1, and leptin levels, all of which temporarily stimulate growth plate activity. This can make a heavier child look taller early on — but the same hormonal environment also accelerates bone maturation, so growth plates close sooner than they should.
How do fat cells cause early puberty?
Fat cells contain an enzyme called aromatase that converts androgens into estrogen. Children who carry excess weight produce more estrogen than expected for their age. Elevated estrogen is a potent signal for puberty onset and for growth plate closure, which is why childhood obesity and early puberty so often occur together.
At what point should I have my child's bone age checked?
If your child is noticeably taller than same-age peers but growth seems to be slowing, or if puberty signs appear earlier than expected (before age 8 in girls, before age 9 in boys), a bone age X-ray is worth discussing with a pediatric specialist. Bone age assessment can reveal whether the growth plates are maturing ahead of schedule and how much height potential remains.
References
- The Effect of Childhood Obesity on Growth: Interpretation of Growth Hormone Provocation Tests. Hormone research in paediatrics. 2026. PubMed
- Childhood obesity and the timing of puberty. Trends in endocrinology and metabolism: TEM. 2009. PubMed · DOI
- Effects of obesity on human sexual development. Nature reviews. Endocrinology. 2012. PubMed · DOI
- Early and late weight gain and the timing of puberty. Molecular and cellular endocrinology. 2006. PubMed · DOI
- Impact of obesity on female puberty and pubertal disorders. Best practice & research. Clinical obstetrics & gynaecology. 2023. PubMed · DOI