The Unexpected Thief Behind Slow Growth
When allergies affect child growth, most parents are caught completely off guard. You have done everything right — nutritious meals, consistent bedtimes, daily outdoor play — yet your child keeps falling behind peers on the height chart. The culprit may not be diet or sleep habits at all. Two silent disruptors, allergies and chronic low-grade inflammation, are increasingly recognized by growth specialists as significant drains on a child's height potential.
The body runs two energy-hungry systems in parallel: growth and immune defense. When allergens or persistent inflammation keep the immune system in a constant state of high alert, resources get redirected away from the growth plates. Think of it as a fixed budget being spent in two departments — the more the immune department demands, the less is left for the growth department. Understanding this competition is the first step toward addressing it.
How Cytokines and Cortisol Block the Growth Plate
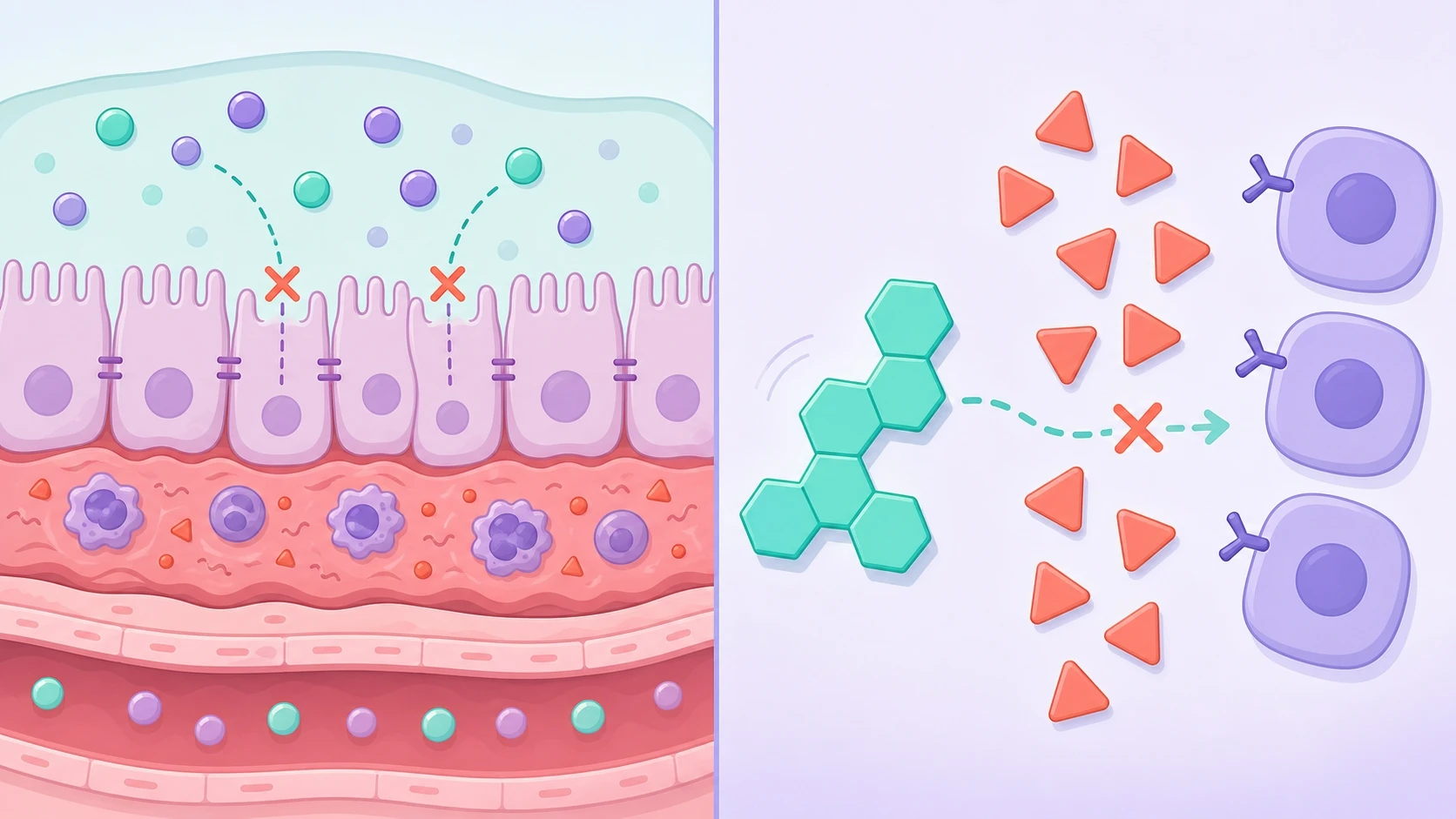
When the body is exposed to allergens or is caught in a cycle of chronic inflammation, immune cells release signaling proteins called cytokines. These molecules do more than trigger local redness or itching — they actively interfere with growth hormone secretion and can blunt the growth plate's response to the hormone even when levels appear normal on a blood test.
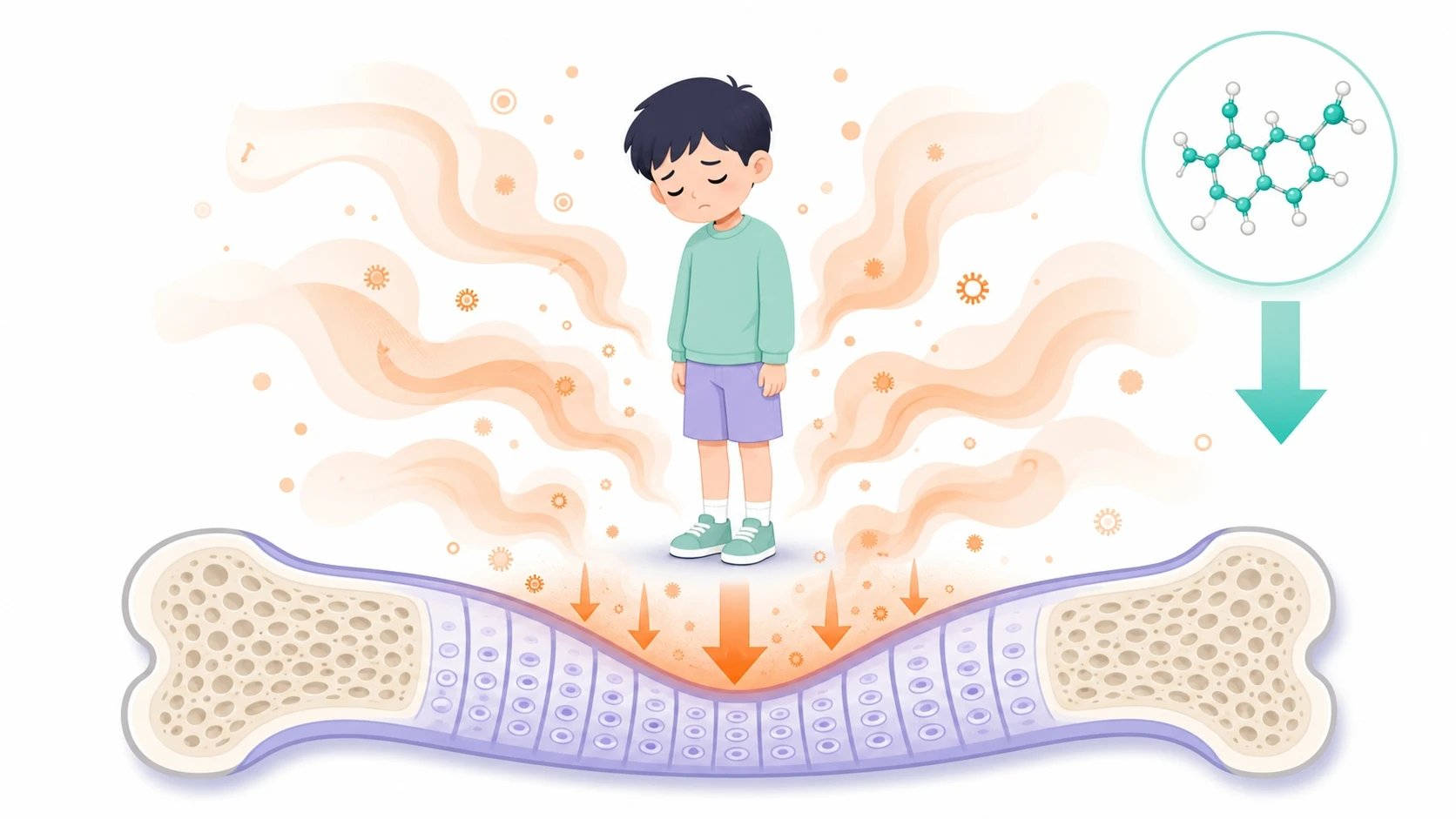
Alongside cytokines, the stress of a perpetually activated immune system prompts the adrenal glands to produce cortisol. Chronic inflammation stunts height in part because elevated cortisol is a well-documented antagonist of growth hormone: it suppresses growth plate cell activity, slows bone mineralization, and accelerates the narrowing of cartilage zones where longitudinal bone growth occurs. This hormonal tug-of-war is a key mechanism behind atopy and short stature observed in clinical practice — children with poorly managed allergic conditions often track at lower height percentiles than their genetic potential would predict.
Atopic Dermatitis, Rhinitis, and Asthma — Three Pathways to Shorter Stature
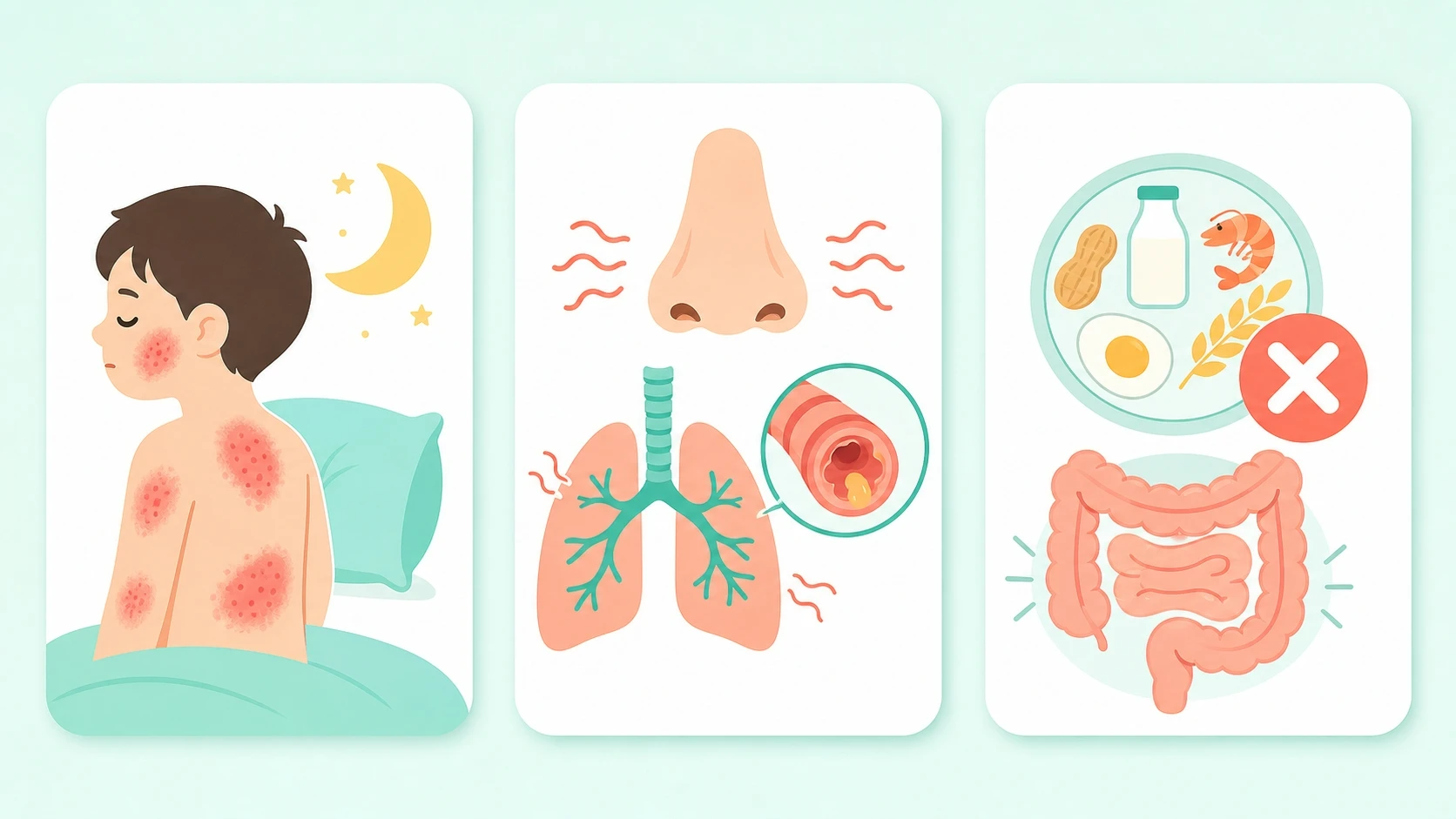
Atopic dermatitis causes relentless nighttime itch that fragments sleep — the very window when the brain releases the largest pulse of growth hormone. Repeated sleep disruption means repeated missed peaks, and the cumulative deficit compounds over months and years. Additionally, the damaged skin barrier invites frequent infections that further tax the immune system.
Allergic rhinitis and asthma force the airway into a state of chronic inflammation, directly linking airway allergies and chronic inflammation stunting height through two routes: poor oxygenation during sleep and elevated whole-body inflammatory load. When a child struggles to breathe at night, deep sleep stages shorten, growth hormone pulses decrease, and morning cortisol tends to rise.
Food allergy and growth in children intersect through the gut. Allergic reactions in the intestinal lining impair absorption of calcium, vitamin D, zinc, and protein — all raw materials the growth plate depends on. Dietary restrictions imposed to avoid trigger foods can create additional nutritional gaps if not carefully managed.
Chronic Low-Grade Inflammation: The Invisible Growth Blocker
Unlike an acute allergic flare, chronic low-grade inflammation produces no obvious hives or sneezing. It can simmer silently for months, triggered by ultra-processed foods, fine particulate air pollution, irregular sleep schedules, and unmanaged emotional stress. Because it lacks a dramatic presentation, parents rarely connect it to a child who simply grows more slowly than expected.
Internally, the picture is clear: chronically elevated inflammatory markers keep the immune system partially activated around the clock. The sustained cortisol signal this generates progressively slows chondrocyte (growth cartilage cell) proliferation inside the growth plates. Long-term studies in pediatric populations show that children with elevated C-reactive protein or interleukin-6 in early childhood tend to achieve lower final adult height — a direct demonstration of how chronic inflammation stunts height over time. Identifying and reducing this background inflammation is therefore as important as managing overt allergic disease.
Practical Steps to Protect Your Child's Growth Potential

Identify and manage triggers precisely. Allergy testing — skin prick or specific IgE blood panels — can pinpoint exactly which environmental or food allergens are driving the immune response, allowing targeted avoidance rather than unnecessary dietary restriction.
Adopt an anti-inflammatory diet pattern. Prioritize fresh vegetables and fruit, whole grains, omega-3-rich fish, and fermented foods that support gut microbiome diversity. Limit ultra-processed foods, added sugars, and trans fats — all of which are documented drivers of the chronic low-grade inflammation that blunts growth. For children with confirmed food allergy and growth concerns, a registered dietitian can design a nutritionally complete elimination plan.
Protect sleep architecture. Treat nasal congestion and itch before bedtime. Consider nasal saline rinses, allergen-proof bedding covers, and pediatrician-approved antihistamines when appropriate. A consistent sleep schedule in a cool, dark room supports the deep-sleep stages essential for peak growth hormone secretion.
Reduce environmental inflammatory load. Air purifiers with HEPA filtration, regular vacuuming with HEPA bags, and minimizing exposure to tobacco smoke and diesel particulates can meaningfully lower the background inflammatory burden on a child's immune system.
When to Seek Specialist Support

Home management goes a long way, but some children need a more comprehensive assessment. If your child has a known allergic condition and is consistently tracking below the 25th height percentile for age, growing less than 4 cm per year after age 3, or showing signs of nutritional deficiency despite an apparently adequate diet, a specialist evaluation is worth considering.
Pediatric growth specialists take a multi-system view — assessing bone age alongside allergy history, inflammatory markers, nutritional status, and sleep quality — to build a picture of what may be constraining the child's height trajectory. In some cases, addressing the underlying allergic or inflammatory condition produces a meaningful catch-up growth response. In others, additional interventions targeting the growth axis itself may be appropriate. Either way, early assessment tends to offer more options, since the growth plates remain open for only a finite window of time.
FAQ
Can treating my child's allergies actually help them grow taller?
Effective allergy management can remove a significant burden from the immune system, allowing more metabolic resources to be directed toward growth. Clinical observations suggest that children whose atopic dermatitis or allergic rhinitis is brought under good control sometimes show an improvement in growth velocity. The effect is most pronounced when treatment starts while the growth plates are still open, underscoring the value of early intervention.
How does food allergy affect growth in children differently from environmental allergy?
Environmental allergies — such as dust mite or pollen sensitivity — primarily disrupt growth through sleep fragmentation and systemic inflammation. Food allergies add a nutritional dimension: intestinal allergic reactions damage the gut lining, reducing the absorption of key growth nutrients like calcium, zinc, and protein. Dietary restriction without expert guidance can also create calorie or micronutrient gaps that compound the shortfall.
What is the connection between atopy and short stature?
Atopy refers to the genetic tendency to develop allergic conditions such as eczema, rhinitis, and asthma. Research indicates that children with multiple atopic conditions are more likely to track at lower height percentiles, partly due to sleep disruption, partly due to chronic cortisol elevation, and partly due to the inflammatory cytokines that interfere with growth hormone signaling. Treating the atopic conditions — not just waiting for the child to 'grow out of it' — is associated with better growth outcomes.
References
- Nutritional Status of Children with Short Stature Is Oppositely Associated with Growth Hormone Peak in Stimulation Tests and Insulin-like Growth Factor-1 Concentration. Journal of clinical medicine. 2026. PubMed
- Association between noncow milk beverage consumption and childhood height. The American journal of clinical nutrition. 2017. PubMed · DOI
- Auxology - an update 2025. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2026. PubMed
- Growth and biochemical markers of growth in children with snoring and obstructive sleep apnea. Pediatrics. 2002. PubMed · DOI
- Aromatase Inhibitors Treatment Alone or With GH Increases Final Height in Short-statured Pubertal Boys-Real-world Data. The Journal of clinical endocrinology and metabolism. 2025. PubMed · DOI